|
Moderate iron
deficiency anemia in the treatment of metabolic
syndrome
......................................................................................................................................................................
Mehmet Rami Helvaci (1)
Murat Albayrak (1)
Ozlem Sahin Balcik (1)
Harika Celebi (1)
Abdulrazak Abyad (2)
Lesley Pocock (3)
(1) Professor of Internal
Medicine, M.D.
(2) Middle-East Academy for Medicine of Aging,
Chairman, MD, MPH, MBA, AGSF
(3) medi-WORLD International
Correspondence:
Mehmet Rami Helvaci, M.D.
07400, ALANYA, Turkey
Phone: 00-90-506-4708759
Email: mramihelvaci@hotmail.com
|
ABSTRACT
Background: Body mass index (BMI),
weight, and height may be due to various
hereditary and environmental factors.
Material and methods: Age and sex-matched
cases with a hematocrit value of less than
30% were collected into the first, less
than 36% into the second, less than 40%
into the third, and 40% or greater into
the fourth groups of patients.
Results: The study included 108 anemia patients
(101 females) with a mean age of 34.7 years
(range 15-68). The anemia cases were mainly
iron deficiency anemia and/or thalassemia
minors. When we compared the first group
with the second, the BMI and weight were
significantly retarded in the first group
(23.6 versus 26.9 kg/m2, p= 0.005 and 61.3
versus 69.9 kg, p= 0.008), whereas there
were nonsignificant differences between
the second, third, and fourth groups for
both (p>0.05 for all). Although there
was significantly retarded BMI and weight
in the first group, body heights were similar
in the four groups (p>0.05 for all).
Conclusion: Although the BMI and weight
can be affected by moderate anemia, the
height may strongly be determined by heredity.
Since the excess weight may be a significant
underlying cause of the metabolic syndrome,
and the metabolic syndrome shortens human
lifespan significantly, and there is no
case with shortened survival due to iron
deficiency anemia and/or thalassemia minors,
an iatrogenic and moderate iron deficiency
anemia with frequent blood donation may
prolong human survival by decreasing the
BMI and weight in the overweight and obese
individuals.
Key words: Iron deficiency anemia,
thalassemia minor, metabolic syndrome, weight,
height
|
Body mass index (BMI), weight,
and height may be due to effects of various hereditary
and environmental factors. Many studies assume
that genes may be importantin these factors, and
there is a common agreement that parents' heights
affect the stature of the children (1, 2). External
factors may also play a role on the body weight
and height. It was shown in a previous study that
rural and urban living conditions may cause up
to a 30% of difference in weight and a 12% of
difference in height (3). But there is still little
known about genetic and environmental control
of the BMI, weight, and height. On the other hand,
anemia is defined as a reduction of hemoglobin
in the red blood cells (RBCs), and millions of
people suffer from it in the world. Iron deficiency
anemia and alpha and/or beta thalassemia minors
are the most common types of anemia seen in the
world. Hemoglobin is the iron-rich protein of
the RBCs that carries oxygen from the lungs to
the body. The final consequence is a decrease
in the blood's ability to carry oxygen to the
body and supply it with the energy that it needs.
So the important body processes including cell
building, tissue repair, and muscular activity
slow down in case of iron deficiency anemia. Dizziness
and a decrease in mental acuity may result due
to the lack of oxygen to the brain and heart failure
due to the increased work of heart. Loss of appetite,
palpitation, difficulty in concentration, depression,
fatigue, coldness of extremities, pallor (reduced
amount of oxyhemoglobin in the skin and mucous
membranes), brittle nails, cessation of menstruation,
breathlessness on exertion, glossitis (inflammation
of the tongue), and angular cheilitis (inflammation
of mouth corners) are the other common symptoms
and signs seen with the iron deficiency anemia.
All of the above symptoms are related to the decreased
cell turnover and increased work of heart due
either to the decreased oxygen supply or to the
decreased iron supplement of tissues. We tried
to understand possible effects of various hematocrit
values on the BMI, weight, and height.
The study
was performed in the Hematology Polyclinics of
the Mustafa Kemal University and Diskapi Yildirim
Beyazit Education and Research Hospital on routine
check up patients between August 2009 and August
2010. The medical history of all cases including
already used medications was learnt, and a routine
check up procedure was performed. Insulin using
diabetics and patients with devastating illnesses
including malignancies, chronic renal diseases,
cirrhosis, hyper- or hypothyroidism, heart failure,
thalassemia intermedia and major, sickle cell
diseases (SCDs), and autoimmune hemolytic anemias
were excluded to avoid their possible effects
on the BMI, weight, height, or hematocrit values.
Body weights and heights were measured, and the
BMI of each case was calculated by the physicians
instead of verbal expressions, since there is
evidence that heavier individuals systematically
underreport their weight relatively to the lighter
ones (4). Weight in kilograms is divided by height
in meters squared (5). Iron deficiency anemia
and thalassemia minors were diagnosed with serum
iron, iron binding capacity, ferritin, and hemoglobin
electrophoresis performed via high performance
liquid chromatography. Age and sex-matched cases
with a hematocrit value of less than 30% were
collected into the first, less than 36% into the
second, less than 40% into the third, and 40%
or greater into the fourth group. Finally, the
four groups were compared in between according
to the mean BMI, weight, and height. Mann-Whitney
U Test, Independent-Samples T Test, and comparison
of proportions were used as the methods of statistical
analyses.
The study included 108 anemia
patients (101 females) with a mean age of 34.7
years (range 15-68). The anemia cases were mainly
iron deficiency anemia and/or thalassemia minors.
The female predominance of the anemia cases (93.5%)
is due to the menorrhagia induced iron deficiency
anemia in this age group. The mean hematocrit
values were 23.4, 32.6, 37.7, and 41.6%, respectively,
in the groups. The mean corpuscular volume (MCV)
values were 58.3, 71.4, 83.3, and 85.5 fL, respectively,
in them. When we compared the first group with
the second according to the mean BMI and weight,
both of them were significantly retarded in the
first group (23.6 versus 26.9 kg/m2, p= 0.005
and 61.3 versus 69.9 kg, p= 0.008, respectively),
whereas there were nonsignificant differences
between the second, third, and fourth groups for
both (25.1, 26.6 kg/m2 and 66.6, 71.8 kg, respectively,
p>0.05 for all). Interestingly, although the
significantly retarded values of the mean BMI
and weight in the first group, the mean heights
were similar in the four groups (161.0, 160.7,
162.1, and 163.1 cm, respectively, p>0.05 for
all) (Table 1).
Table 1: Characteristics of the study cases
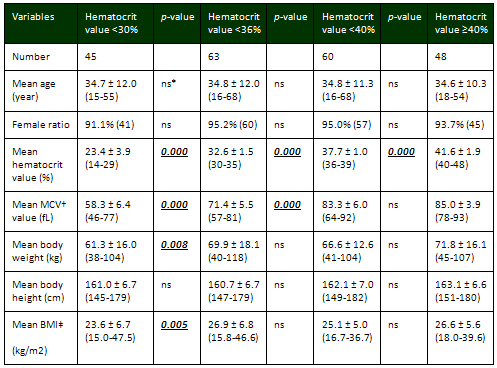
*Nonsignificant (p>0.05) †Mean corpuscular
volume ‡Body mass index
Iron deficiency anemia is the
most common type of anemia in the world, and mostly
seen in children due to the increased iron requirement
in growth and in women due to the increased iron
requirement in pregnancy, lactation, and menstruation.
For instance, nine to 11% of adolescent girls
and women in childbearing age have iron deficiency,
compared with less than 1% of young men in the
United States (6). Similarly, the significantly
lower MCV values of the anemia patients in the
present study also indicate that the majority
of cases with anemia are secondary to iron deficiency
and/or thalassemias because both are the most
common causes of microcytic anemias in the world.
The female predominance (93.5%) and young mean
age of the anemia patients (34.7 years) of the
present study is due to the menorrhagia induced
iron deficiency anemia since iron deficiency anemia
can be caused by insufficent dietary intake of
iron, insufficient absorption of iron, or blood
loss which is often caused by menstruation. Iron
deficiency anemia induced sign and symptoms may
be due to the tissue hypoxia and/or iron deficiency
alone since iron takes additional roles in the
various tissues and enzymes in the body. Glossitis,
angular cheilitis, koilonychia (spoon-shaped nails),
and dysphagia due to formation of esophageal webs
in the Plummer-Vinson syndrome may be some of
the indicators of various roles of iron other
than the hemoglobin in the body. Thus moderate
anemia induced retarded BMI and weight in the
present study may also be secondary to the various
roles of iron in tissues and enzymes other than
the hemoglobin alone. Thalassemias are the other
most common causes of microcytic anemia in the
world, particularly in the Mediterranean region.
They are autosomal recessively inherited disorders.
Normal hemoglobin is composed of two pairs of
alpha and beta globin chains. Alpha thalassemias
result in a decreased alpha globin synthesis,
causing an excess of beta chains in adults. The
excess beta chains form unstable tetramers (called
hemoglobin H) which have abnormal oxygen dissociation
curves. Whereas in beta thalassemias, excess alpha
chains bind to the RBC membranes causing membrane
damage and they form toxic aggregates at high
concentrations. Generally, thalassemias are prevalent
in populations that evolved in humid climates
where malaria is endemic since thalassemias protect
these people from malaria due to the easy degradation
of the RBCs. Alpha and beta thalassemias are also
frequent in Turkey, especially in the Mediterranean
region, and most of the cases with anemia in the
present study have alpha thalassemias and/or beta
thalassemias and/or iron deficiency anemia. Pathophysiologic
mechanisms of the lower BMI and weight in the
thalassemia cases may include anemia induced tissue
hypoxia, increased cardiac activity, increased
bone marrow activity, and increased splenic activity.
In this field, iron deficiency anemia and thalassemia
cases must be researched separately with increased
number of cases in further studies. But it is
obvious that neither the iron deficiency anemia
nor the alpha and/or beta thalassemia minors do
not shorten lifespan of the human being.
Normally the BMI and weight may
be determined by a complex network of hormonal,
nutritional, physical, and genetic factors. For
instance, approximately 70 genes may take role
in the regulation of bone mass (7), and some genes
were shown to affect both the BMI and bone geometric
parameters (8). The same results were also shown
in animals that the results indicate substantial
additive genetic control of Brahman body weight
to hip height ratio (9). Leptin is a hormone produced
mainly by adipocytes and it acts centrally to
control the body weight (10). Leptin is also expressed
on osteoblasts and acts as a skeletal growth factor
and promotes bone mineralization (11, 12). The
pleiotropic effect of leptin on the BMI and bone
geometry may also be supported by the evidence
of genetic correlation of leptin with the BMI
and bone geometry (13). On the other hand, the
body length growth velocity was found not to be
affected by genes in some studies (14). Whereas
we detected in the present study that although
the significantly retarded BMI and weight in the
moderate anemia (p< 0.05 for both), the heights
were similar in all groups without any effect
of anemia (p>0.05 for all). Similarly, in a
previous study (15) performed on 122 patients
(58 females) with the SCDs with a mean age of
28.6 years, although the BMI and weight were significantly
retarded in the SCDs cases (24.9 versus 20.7 kg/m2
and 71.6 versus 57.8 kg, p= 0.000 for both) probably
due to the accelerated vascular endothelial damaging
process initiated at birth; the heights were similar
in the SCDs and control groups (166.1 versus 168.5
cm, respectively, p>0.05) probably due to its
hereditary nature.
Chronic endothelial damage may
be the major cause of aging, morbidity, and mortality
by causing disseminated tissue hypoxia all over
the body. Some of the well-known accelerators
of the inflammatory process are physical inactivity
induced excess weight, smoking, and alcohol for
the development of irreversible consequences including
obesity, hypertension (HT), diabetes mellitus
(DM), cirrhosis, peripheric artery disease (PAD),
chronic obstructive pulmonary disease (COPD),
chronic renal disease (CRD), coronary artery disease
(CAD), mesenteric ischemia, osteoporosis, and
stroke, all of which terminate with early aging
and death. They were researched under the title
of metabolic syndrome in the literature, extensively
(16, 17). The metabolic syndrome may be the most
common type of vasculitis in the world, and leading
cause of aging, morbidity, and mortality in human
beings. Much higher blood pressure (BP) of the
afferent vasculature may be the major underlying
cause by inducing recurrent injuries on endothelium.
Thus the term of venosclerosis is not as famous
as atherosclerosis in the literature. Secondary
to the chronic endothelial inflammation, edema,
and fibrosis, vascular walls become thickened,
their lumens are narrowed, and they lose their
elastic natures that reduce blood flow and increase
systolic BP further. Although early withdrawal
of causative factors may prevent final consequences,
after development of obesity, HT, DM, cirrhosis,
PAD, COPD, CRD, CAD, mesenteric ischemia, osteoporosis,
or stroke, endothelial changes cannot be reversed
completely due to their fibrotic natures (18,
19). Other chronic inflammatory processes including
SCDs, rheumatologic disorders, prolonged infections,
and cancers may accelerate the process. Finally
it is obvious that the metabolic syndrome terminates
with a significantly shortened survival in human
being (20).
As a conclusion, although the BMI and weight can
be affected by moderate anemia, the height may
strongly be determined by heredity. Since the
excess weight may be a significant underlying
cause of metabolic syndrome, and the metabolic
syndrome shortens human lifespan significantly,
and there is no case with shortened survival due
to the iron deficiency anemia and/or thalassemia
minors, an iatrogenic and moderate iron deficiency
anemia with frequent blood donation may prolong
human survival by decreasing the BMI and weight
in the overweight and obese individuals.
1. Rona RJ, Chinn S. Genetic
and environmental influences on growth. J Med
Screen 1995; 2: 133-139.
2. Preece MA. The genetic contribution to stature.
Horm Res 1996; 45: 56-58.
3. Habicht JP, Martorell R, Yarbrough C, Malina
RM, Klein RE. Height and weight standards for
preschool children. How relevant are ethnic differences
in growth potential? Lancet 1974; 1: 611-614.
4. Bowman RL, DeLucia JL. Accuracy of self reported
weight: a meta-analysis. Behav Ther 1992; 23:
637-635.
5. Third Report of the National Cholesterol Education
Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults
(Adult Treatment Panel III) final report. Circulation
2002; 17:106: 3143-3421.
6. Looker AC, Dallman PR, Carroll MD, Gunter EW,
Johnson CL. Prevalence of iron deficiency in the
United States. JAMA 1997; 277: 973-976.
7. Khoury MJ. Genetic epidemiology and the future
of disease prevention and public health. Epidemiol
Rev 1997; 19: 175-180.
8. Xu H, Xiong DH, Xu FH, Zhang YY, Lei SF, Deng
HW. Association between VDR Apal polymorphism
and hip bone mineral density can be modified by
body mass index: a study on postmenopausal Chinese
women. Acta Biochim Biophys Sin (Shanghai) 2005;
37: 61-67.
9. Riley DG, Coleman SW, Chase CC Jr, Oslon TA,
Hammond AC. Genetic parameters of body weight,
hip height, and the ratio of weight to hip height
from random regression analyses of Brahman feedlot
cattle. J Anim Sci 2007; 85: 42-52.
10. Considine RV, Sinha MK, Heiman ML, Kriauciunas
A, Stephens TW, Nyce MR, et al. Serum immunoreactive-leptin
concentrations in normal-weight and obese humans.
New Engl J Med 1996; 334: 292-295.
11. Reseland JE, Syversen U, Bakke I, Qvigstad
G, Eide LG, Hjertner O, et al. Leptin is expressed
in and secreted from primary cultures of human
osteoblasts and promotes bone mineralization.
J Bone Miner Res 2001; 16: 1426-1433.
12. Ducy P, Amling M, Takeda S, Priemel M, Schilling
AF, Beil FT, et al. Leptin inhibits bone formation
through a hypothalamic relay: a central control
of bone mass. Cell 2000; 100: 197-207.
13. Livshits G, Pantsulaia I, Trofimov S, Kobyliansky
E. Genetic variation of circulating leptin is
involved in genetic variation of hand bone size
and geometry. Osteoporosis Int 2003; 14: 476-483.
14. Livshits G, Peter I, Vainder M, Hauspie R.
Genetic analysis of growth curve parameters of
body weight, height and head circumference. Ann
Hum Biol 2000; 27: 299-312.
15. Helvaci MR, Kaya H. Effect of sickle cell
diseases on height and weight. Pak J Med Sci 2011;
27: 361-364.
16. Eckel RH, Grundy SM, Zimmet PZ. The metabolic
syndrome. Lancet 2005; 365: 1415-1428.
17. Helvaci MR, Kaya H, Sevinc A, Camci C. Body
weight and white coat hypertension. Pak J Med
Sci 2009; 25: 6: 916-921.
|
